Sun, 29 December 2019
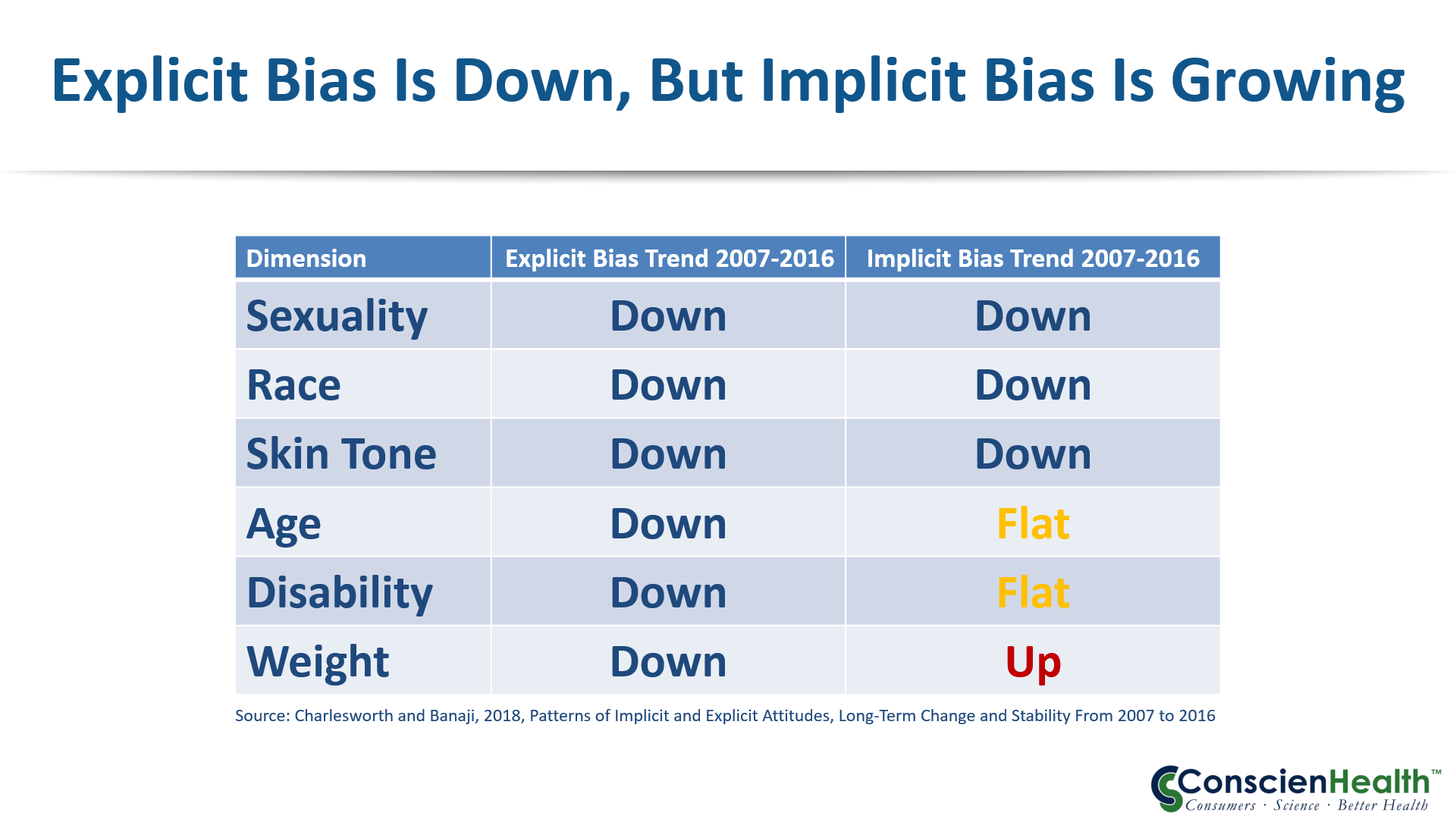
In this episode I bring you my conversation with Ted Kyle, RPh, MBA. Ted founded ConscienHealth in 2009. He is a pharmacist and healthcare innovation professional who works with health and obesity experts for sound policy and innovation to address obesity. He serves on the Board of Directors for the Obesity Action Coalition, advises The Obesity Society on advocacy, and consults with organizations addressing the needs of people living with obesity. His widely-read daily commentary, published at conscienhealth.org/news, reaches an audience of more than 15,000 thought leaders in health and obesity. His peer-reviewed publications focus upon weight bias and policy related to health and obesity. As such, Ted is perfectly positioned to share with us his list of the Top 10 Milestones in Obesity and Health over the past 10 years. Discussed in this episode, # 10-# 1: 10. The Rise of ObesityWeek: We discuss what is ObesityWeek and why does this conference matter. 9. The Mediterranean Diet Hits a Speed Bump: In 2018 the original authors of the PREDIMED study audited the study’s data and execution and they found problems. For about 14 percent of the study’s 7,447 subjects, assignment to a treatment group was not random. Taking those problems into account, they still found lower rate of cardiovascular events for people in the Mediterranean diet groups (compared to a lower-fat diet). But the bold claim of cause and effect evaporated. The original conclusions said the diet “reduced the incidence” of cardiovascular events. The new conclusion says “the incidence was lower.” This difference might seem small but it’s the difference between causality and association. 8. Plants Are IN, But Carbs Are OUT: As demonstrated by the new Dietary Guidelines for Americans in 2020. 7. Vibrant Support and Advocacy for People with Obesity: The rise of the Obesity Action Coalition. 6. Sugar Is Poison: Dr Robert Lustig's Sugar-is-Toxic video 5. A Whole New Specialty for Obesity Care: American Board of Obesity Medicine came into existence. 4. Surgery for Diabetes: Understanding that Bariatric Surgery is an endocrine surgery that changes the hormonal communication between the gut, adipose (fat) tissue, and the brain. The logic is inescapable. Type 2 diabetes is a cruel, progressive disease that slowly, but surely destroys a body from the inside out. Strokes, heart disease, amputations, organ failure – they’re all part of a bleak picture. Intensive medical care can slow it down. But metabolic surgery can put it into remission. Three years ago (2016), a remarkable consortium of 45 expert organizations endorsed metabolic surgery for type 2 diabetes. And yet, 97 percent of people who might benefit still don’t receive metabolic surgery. 3. New Drugs for Obesity Treatment: Liraglutide (Saxenda), Naltrexone & Bupropion (Contrave), Phentermine & Topiramate (Qsymia), and Lorcaserin (Belviq), with more coming. 2. Sleeves Take Over from Bands: Bands peaked in 2007. As of 2018 Vertical Sleeve Gastrectomy is the #1 procedure of all bariatric surgeries. 1. Less Explicit Bias: Bias comes from selective blindness to facts. Explicit bias refers to attitudes and beliefs we have about a person or group on a conscious level. Implicit bias refers to thoughts and feelings we hold without conscious awareness regarding a person or group. Some of the more common biases we can hold against a person are based on their weight, sexuality, race, age, skin tone, or disability. The risks of implicit and explicit bias is that people become sicker because of denial and inaction. Less (NONE!) of both types of biases would be better but less explicit bias is certainly a start. Thanks for Listening! Support the podcast at either: Patreon or PayPal Connect with Ted Kyle: ConscienHealth.org, LinkedIn, Twitter, Facebook, Instagram, email: Ted.Kyle@conscienHealth.org Connect with Reeger Cortell: Facebook, Twitter, Instagram, email: reeger@weightlosssurgerypodcast.com
Direct download: 10_Years_10_Milestones_in_Obesity_and_Health_with_Ted_Kyle.mp3
Category:general -- posted at: 4:59pm PDT |
Mon, 2 December 2019
In this episode I bring you obesity and bariatric surgery research scientists, Dr. Randy Seeley. If you have been a longtime listener of the podcast then you will likely remember Dr Seeley from Episode 34 where he helped us understand the theory of Set-point for body fat mass and Episode 56 where we did a deeper dive into the biology of body weight. This time I bring Dr Seeley back to help get us get up to speed on what research has learned about bile acid metabolism in general and as it relates to obesity and bariatric surgery specifically. We also talk some about the “bugs” of the gut, also known as the gut microbiome. Additionally, we chat about what his research is revealing about sleep apnea and the gut, as well as iron metabolism after bariatric surgery. And just for fun, there is a cameo appearance of his dog, Ziggy. After all that, as always, I share with you my concluding thoughts about the episode. But before I cut to the episode I want to tell you about the sponsors who make this podcast possible. That would be you, my listeners. You support the podcast every time you tell someone about it, share it, rate it, and if you are able, by becoming a patron. You can become a patron of the podcast at either Patreon or PayPal where you have the option of offering either recurring monthly support or one time support. Click on Patreon or PayPal to be taken to their sites or you can find the links in the upper right-hand corner of my website, WeightLossSurgeryPodcast.com If you are already a supporter of the podcast in any capacity, thank you ever so much. Discussed In This Episode: Randy Seeley, PhD is a Professor of Surgery, Internal Medicine, and Nutritional Science at the University of Michigan. One area his research focuses on is trying to find and understand the molecular signals that come from the gut in general and how bariatric surgery changes those signals to support a reduction in hunger and weight. What is Bile: Made in the liver and stored in the gallbladder. When we eat foods with lipids (fat). Bile is released at the beginning of the small intestines. Unused bile acids are reabsorbed into the blood at the bottom part of the small intestine and are brought back up to the liver to be used again. Roux-en-Y Gastric Bypass (RYGB) patients have higher levels of bile circulating in their blood compared to non-RYGB patients. Interestingly, animal models and humans who undergo Vertical Sleeve Gastrectomy (VSG) also have increased blood levels of bile, even though the intestines are not changed in VSG, only the stomach is changed. The reason is that the liver stops taking up, recycling, as much bile. Somehow the liver knows that part of the stomach has been removed. Figuring out if this matters, led Dr Seeley to dig deeper into the role of bile acids. It turns out that bile acids not only work to break down dietary fats that are eaten. Bile also acts a Hormone (A hormone is a chemical signal that is released in one area of the body and communicates with another part of the body by binding with a receptor.) One of the important receptors that bile binds to is FXR. FXR has been linked to many aspects of metabolism. In order to determine what role FXR plays in the binding of bile, Dr Seeley’s lab created genetically alerted rodents who no longer have the FXR receptor. They then performed VSG on the rodents. The theory was that if elevated plasma bile acids (bile in the blood) mattered to why the surgery works, then you would expect that animals who no longer have the FXR receptor would not respond as well to the surgery. That is exactly what happened. Ultimately, the animals without FXR did not have suppression of food intake even though it has a smaller stomach. Additionally, the FXR-missing animals did not have blood glucose level improvement. Why does this matter? Dr Seeley argues the more we can identify these specific molecular pathways by which bariatric surgery works the better we can understand who might benefit from the surgery and ultimately, perhaps, we can make surgery a thing of the past because we have figured out treatments that are just as beneficial but not as invasive as surgery. Bile acid is not just one thing. There are different types of bile acids, or as Dr Seeley likes to call it, a gemisch (meaning mixture) of bile acids. Most basically there are Primary Bile Acids, which are made by the liver and there are Secondary Bile Acids, which are altered, changed, by the bacteria in the gastrointestinal track. Some of the primary and secondary bile acids turn on and off different receptors including FXR. Studies in humans are more complicated because as Dr Seeley points out, people don't want to line up to have their FXR receptor deleted. However, the biology between rodents and people is translatable. My questions to Dr Seeley: Are the changes in bile acid metabolism independent of weight loss or are they due to lowered body fat stores, or reduced calorie intake, or different calories, or increased physical activity, etc? To answer this question Dr Seeley discusses a study completed at Washington University, by Samuel Klein, MD who compared people who had gastric band, VSG, and RYGB. He compared people who did well with the band (lost similar amounts of weight to VSG and RYGB people) to people who had VSG or RYGB. What he found is that even though the gastric band patients had lost similar amounts of weight, their bile acids had not changed. The change in bile acids are only seen in the VSG and RYGB patients. But how does the liver know to not uptake bile and why? We don't know the answer, yet. Bugs: My Question: What role do the bugs (bacteria) living inside the gut have to play in any of this? Dr Seeley points out that there is some controversy around the question of if and how much the microbiome influences weight. Here is what we know after surgery, the bugs in the poop are different after RYGB than before. What we don't know is if the changes in the gut bacteria are a knock-on effect (a consequence) of bariatric or are they something that helps drive (create) some of the biological changes of the surgery (chicken or egg question)? After all, the bugs can change the bile acids and bile acids can change the bugs. Again, we don't know that answers, yet. Dr Seeley’s long-term research goal is to recapitulate (mimic or repeat) the benefits of bariatric surgery without having to actually perform bariatric surgery. He highlights that it is not realistic to expect that all the multiple millions of people who are affected by obesity can or will have bariatric surgery. Therefore, research needs to help us find alternative treatments that are as effective. My question: Are these changes durable? Do they last? For some people the changes are durable but the question is for whom are the changes durable? Dr Seeley talks about type 2 diabetes (T2D), stating that it is well known that bariatric surgery helps treat T2D. However, it is also known that for many people, their T2D will return at some point after bariatric surgery. We agreed that the longer a person had their T2D before bariatric surgery, the greater the chance their T2D will come back after bariatric surgery, but we cannot say exactly when nor how significantly their T2D will return. The fact that there is a high chance of recurrence is not a question of if we should do bariatric surgery, but rather when (the sooner the better?) Sleep Apnea: Another example of how bariatric surgery helps with biology is related to obstructive sleep apnea (OSA). Many people who are affected by obesity also have OSA and are on or should be on CPAP therapy. It is known that OSA improves after bariatric surgery. The question is why? To attempt to answer this question, Dr Seeley started thinking about why do people affected by obesity even get OSA? The notion that fat around the airway causes the airway to collapse when you lay down depending on which way you lay down never made sense to Dr Seeley. So he tested this on rodents by placing the rodents in a special chamber called a plethysmograph (an instrument that measures the change in volume within an organ or whole body). While the animal is in the chamber the researchers can also manipulate the gas mixture (O2 and CO2). When the researchers raised the amount of carbon dioxide in the chamber and the animal responds by breathing harder, AKA the Hypercapnic Ventilator Response (HVR). They then took rodents who had obesity and found that as the CO2 level in the chamber went up, the rodents HVR went down, their drive to breath is lower. They then performed VSG on the rodents and found that the HVR, the drive to breath, normalized again, independent of weight! This led them to conclude that bariatric surgery changes the drive to breath by showing us that there is intimate involvement from our GI tract relating to our HVR and drive to breathe. Iron Metabolism: Dr Seeley’s research is next leading him to study iron and bariatric surgery. It is a well-known fact that after bariatric surgery iron levels decline in both humans and in research rodents. In researching why this may be, it appears that the rodents’s body wants have a lower iron level. However, it is not just because there is lower iron absorption after bariatric surgery. It also appears that the system, the animal’s body, wants to maintain a lower iron level. Why and how does the body know? More research is needed to answer this question. So in summary, there are benefits with bariatric surgery, we know a tiny portion of them, we know the vast majority of people will reap benefits, but exactly how much and why, we’re still figuring out. Concluding Thoughts So there you have it… is it all clear now? Ok, full disclosure, I realize some of you may be thinking there you have what? After all, it could be easily argued that this episode leaves us all with more questions than answers. And it is hard to make decisions, such as should a person have bariatric surgery and which procedure when all you have are more questions, not answers. Honestly my intent in bringing you this episode was not to answer the big questions, to take the 30 thousand foot view; But rather the opposite, to look very close and get really, really specific. My goal was to help show you in one conversation with one fun and wicked smart scientist, a tiny fraction of some of the research that is happening 24/7, 365 days a year, year after year. All of which is occurring to help us understand the How and Why of a question we actually already know the answer to. That answer being that for most people bariatric surgery works really well. When most people have bariatric surgery they lose weight, the majority of that weight being fat mass. We have known this fact for many, many years. But how and why bariatric surgery works, these are the questions that science is constantly attempting to answer. It is true that in many ways we are reverse engineering the problem. Our ability to safely perform the surgeries has out-paced our deep understanding as to how and why the surgeries work. You will often hear the explanation of bariatric surgery works because of restriction when you make the stomach smaller, and malabsorption when you make the intestines shorter. Which is a little like saying a plan flies because you turn the engine on and speed the plane down a runway. True… These two things are necessary to make a plan fly, but they are not sufficient. You need more than power and a runway to make a plan fly. The same way restriction and malabsorption are necessary parts of bariatric surgery, but we now know because of scientists like Randy Seeley, those two things are not sufficient. There is more going on that makes bariatric surgery work as effectively as it does. But exactly how and why is still being answered, study-by-study. Which brings me to another deeper question, when we get really honest about how much we do and do not know about how and why bariatric surgery works, should we even be performing bariatric surgery? What if in all the research we discover a negative consequence of bariatric surgery that tips the scales towards a much lower efficacy? Should we just put a moratorium on bariatric surgery until we understand more about the how and why it works and the risks and benefits therein? Well, as you might have guessed, I am not in favor of this. Although our bariatric medical and surgical knowledge only spans back to the 1950’s, our understanding the potential health consequences of obesity goes back much farther. To date, bariatric surgery is the most effective treatment we have, even when you factor in what we do not yet know about bariatric surgery. But, having said that, I am continually encouraged by the research scientists like Dr Seeley who are seeking to understand how bariatric surgery works in hopes that broadly an alternative to surgery can be identified and more specifically, we can better determine for whom bariatric surgery will have the most benefit and which surgery. Will have these answers in the next few years? I do not think so. But, when you look at the radical advances science has made just in the last 100 years compared to all scientific advances over human existence, well, I don't think we are doing too badly. And as one final word, here in the United States we just had our national Thanksgiving holiday. I want to take this opportunity to express my gratitude, my thanksgiving, to all of you for listening, for sharing the podcast with others, for writing me at reeger@weightlosssurgerypodcast and for becoming a patron. I do not keep this podcast alive for fame or fortune. I keep it alive because you tell me it makes a difference for you. In this seemingly ever more complicated world, my reasons for keep-on, keeping on, truly against all odds, is simple because of you. You are the reason and I am grateful for you. Never forget, I believe in you. Connecting with Dr Seeley on Twitter Connecting with Reeger
Direct download: Geeking_out_on_BIle_Bugs_and_Bariatric_Surgery_with_Randy_Seeley_PhD_.mp3
Category:general -- posted at: 11:17am PDT |
Sun, 27 October 2019
In this episode I bring you Kelley Gunter. As you are about to hear, Kelley is many things including a woman with a history of obesity who underwent bariatric surgery, specifically Biliopancreatic Diversion with Duodenal Switch in 2002; She is also a writer and author of the autobiography, "You have such a pretty face: A Memoir of trauma, hope, and the joy that follows survival;” She is a motivational speaker; A social media influencer; A music video creative director; A mother to her son Alec; And she is a survivor of childhood sexual abuse whose mission is now to offer hope in times of darkness and healing no matter how deep the scars. In this episode Kelley shares the story of her life before her bariatric surgery and her life since. For many reasons, this is a story that helps us understand the very meaning of the expression “to call on ones courage.” Although we do not discuss sex or sexual abuse in detail, the realities of the sexual violence that was perpetrated against Kelley are a painful but important part of her truth and are central to her healing journey. Therefore this topic does come up as she shares her story. As a result, I want to acknowledge that this episode may be upsetting for some and may not be appropriate for young listeners. Listener discretion is advised. Discussed in this episode:
Connecting with Kelley Gunter
Connecting with Reeger
Direct download: 106_Kelley_Gunter_On_Living_in_the_Truth.mp3
Category:general -- posted at: 8:36pm PDT |
Sun, 29 September 2019
This episode is a little different because I am on the other side of the mic. Rather than asking the questions, I am answering them. Podcaster Don Moe asked me to be a guest on his podcast, Weigh In Radio. I was honored he asked and had fun chatting with him, so much so that I decided to share the episode here with you. If you are not familiar with Don’s podcast, Weigh In Radio, I highly recommend you check it out. He launched his podcast in August of 2018 and to date has published 12 episodes with more coming. Don is someone who is personally affected by obesity and he has included bariatric surgery, specifically Vertical Sleeve Gastrectomy, a.k.a. the Sleeve, as part of his treatment plan. Through both thoughtful interviews and commentaries, his podcast focuses on helping people along their weight loss journey, whether bariatric surgery is part of that journey or not. I am happy to lend my podcast platform to Don if that helps him help more people. His heart is in the right place and his podcast is excellent. I highly recommend you become an active subscriber of Weigh In Radio and the community he is building over there. His podcast is available wherever you listen to podcasts. Discussed in this episode
Direct download: Don_Moe_of_Weigh_In_Radio_Interviews_Reeger.mp3
Category:Podcast Episodes -- posted at: 11:30am PDT |
Thu, 25 July 2019
In this episode I talk with food addiction expert Dr Vera Tarman. Dr Tarman has been working in the field of addiction medicine since 1994 and has been the director of Renascent, an addiction treatment center in Toronto, Canada since 2006. Although she works full-time in all areas of addiction, her particular passion is helping people recover from food addiction. She is the author of the book, “Food Junkies: Recovery from Food Addiction” now in its second edition. We cover a lot of ground in this episode including discussing eating behaviors on a spectrum from normal eating to different types of eating disorders. Then we talk about the similarities and differences between what Dr Tarman identifies as three distinct disease states: Obesity, Emotional Eating, and Chemical Addiction to food. We then focus-in on chemical addiction to food, specifically foods that are created in labs, are highly processed, and are specifically formulated to target the reward centers of our brains. When the reward center in our brain turns on our brain releases neurochemicals that results in thoughts and feelings of, “yes, that tastes especially good and when I eat it I feel, at least temporarily, better, happier, calmer, more fulfilled.’ This sounds great but what is so concerning are the false “promises” that come with highly processed foods and the price we pay is much higher than we realize, including what more and more evidence is showing to be the growing phenomena of chemical addiction to food. Discussed in this episode:
Direct download: What_if_food_addiction_is_part_of_the_problem-_A_talk_with_Dr_Vera_Tarman.mp3
Category:general -- posted at: 9:18pm PDT |
Tue, 25 June 2019
In this episode I chat with Dr Neil Floch. Dr Floch is a bariatric surgeon at Western Connecticut Health Network, now known as NuVance and is in private practice at Fairfield County Bariatrics. This episode starts with Reeger's preamble acknowledging two important anniversaries in the month of June, getting closer to our 5% patron goal (Thank you!), and how to become a patron at either Patreon or PayPal.
Discussed with Dr Floch:
Connect with Dr Floch on Twitter Connect with Reeger: In Kindness, Reeger
Direct download: 103_Making_Connections_with_Bariatric_Surgeon_Dr_Neil_Floch.mp3
Category:general -- posted at: 7:42pm PDT |
Sat, 25 May 2019
In this episode I speak with the wonderful Denise Ratcliffe, DClinPsych. Dr Ratcliffe is a Consultant Clinical Psychologist based in London, United Kingdom. Since 2007, she has specialized in helping people with the psychological issues that may arise before and after bariatric surgery. I invited her on the podcast because she has recently published a book titled, Living with Bariatric Surgery, Managing Your Mind and Your Weight. This is an important book that I wanted to highlight on the podcast because it is filled with helpful insight and great wisdom regarding some of the emotional challenges people can confront before and after bariatric surgery. Throughout the book Dr Ratcliffe offers reality-based tips and strategies to help people overcome those challenges. Discussed in This Episode:
Direct download: 102_Living_with_Bariatric_Surgery_A_Conversation_with_Denise_Ratcliffe.mp3
Category:general -- posted at: 4:57pm PDT |
Mon, 22 April 2019
In this episode I bring you my conversation with Dr Angela Fitch. Dr Fitch is medical doctor at Massachusetts General Weight Center in Boston, Massachusetts. As you are about to hear, her role is very comprehensive in that she provides obesity medicine care for pediatrics and adults seeking medical and bariatric surgery as part of […]
Direct download: 101_Addressing_Weight_Regain_with_Angela_Fitch_MD.mp3
Category:Podcast Episodes -- posted at: 9:01pm PDT |
Thu, 21 March 2019
EPISODE 100! In 2013 when I launched the Weight Loss Surgery Podcast if you had asked me how many episodes I hope to publish I may have dared to say 20. In this episode I want to take a look back over some highlights between episodes 01 and 100. To help me do this I […]
|
Sun, 10 February 2019
In this episode we explore the topic of addiction. Much of the focus is on alcohol because as it pertains to bariatric surgery, that’s what been most significantly studied up to this point. However, as listeners will know, addiction comes in all forms and is certainly not limited to alcohol and drugs. To guide us […]
Direct download: 099_Lets_Talk_About_Addiction.mp3
Category:Podcast Episodes -- posted at: 7:03pm PDT |
Sat, 19 January 2019
This episode brings an important topic to the forefront of the pre- and especially post bariatric surgery journey- the phenomena of Loss of Control (LOC) eating. In order to help us understand what Loss of control eating and is not, I had the pleasure of talking with two experts in the field, clinical psychologists and […]
|
Weight Loss Surgery Podcast - Bariatric / Lap Band / RYGB / Gastric Bypass / Vertical Sleeve Gastrectomy

Categories
generalPodcast Episodes
Archives
OctoberApril
March
February
January
December
October
September
July
June
May
April
March
February
January
December
November
September
June
May
April
February
January
December
October
September
August
July
June
May
April
March
February
January
December
October
September
August
July
June
May
April
March
February
January
December
November
October
September
August
July
June
May
April
March
February
January
December
November
October
September
August
July
June
May
April
March
February
January
December
November
October
September
August
July
June
| S | M | T | W | T | F | S |
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | |
| 7 | 8 | 9 | 10 | 11 | 12 | 13 |
| 14 | 15 | 16 | 17 | 18 | 19 | 20 |
| 21 | 22 | 23 | 24 | 25 | 26 | 27 |
| 28 | 29 | 30 | ||||
Syndication


{kind=link}
